

Streamline CV data collection, interoperability, & reporting through a clinician-focus designed platform for multiple service lines in one independent, relational, patient-centric, procedure-oriented clinical repository including: Cardiology, Electrophysiology, CV Surgery, Vascular Surgery, Thoracic Surgery, Chest Pain, HF, Stroke, ECMO, Custom Research & more!
Key Features
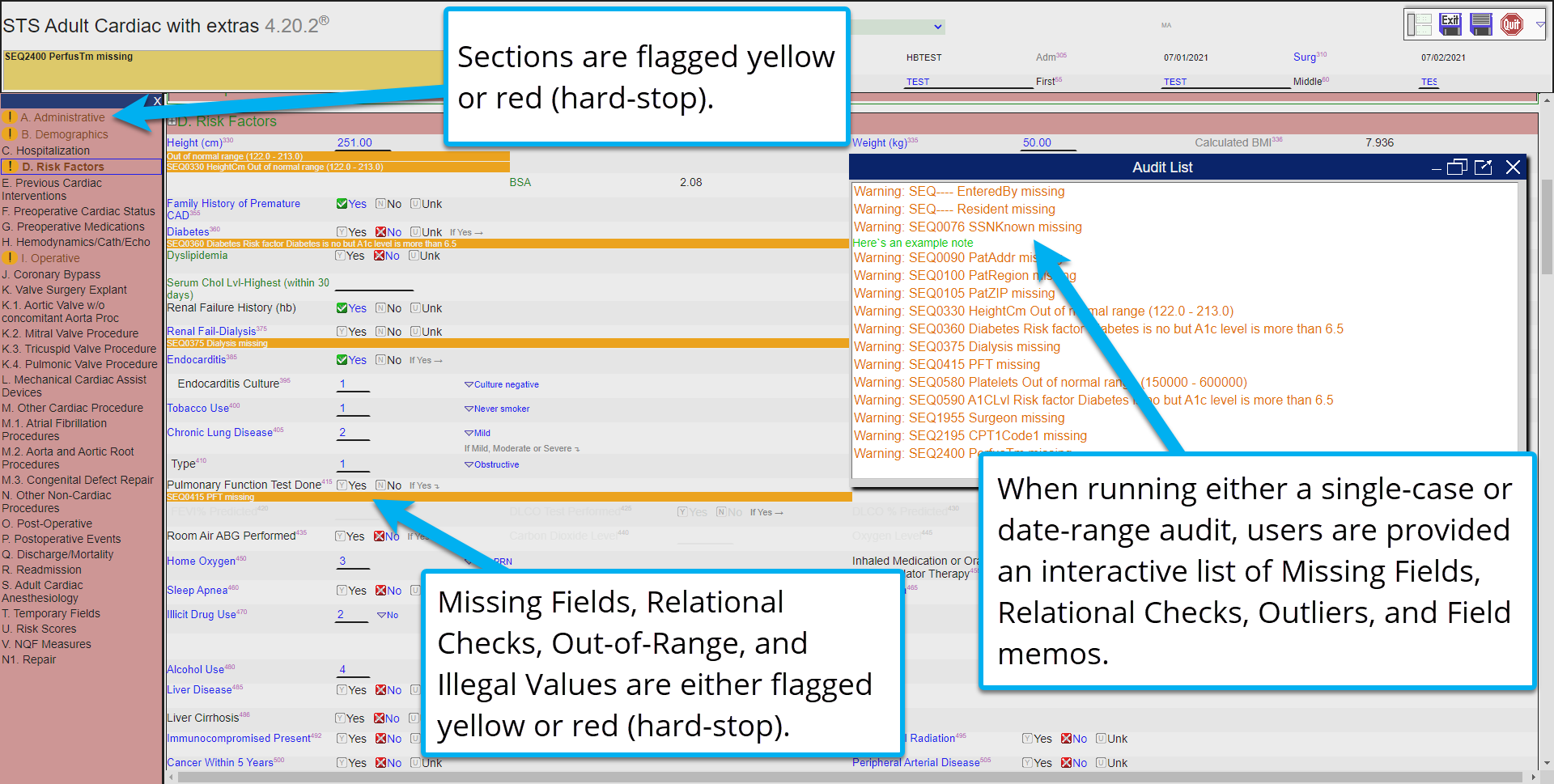
The hbCOR platform provides various pre-harvest data validations that help users ensure data is 100% accurate before submission.
Unlike other vendors, hbCOR data validations happen in real-time, meaning that users receive immediate feedback when a data element may be considered unusual, inconsistent with other variables, or invalid by the registry.
Custom Validation checks are available upon request.
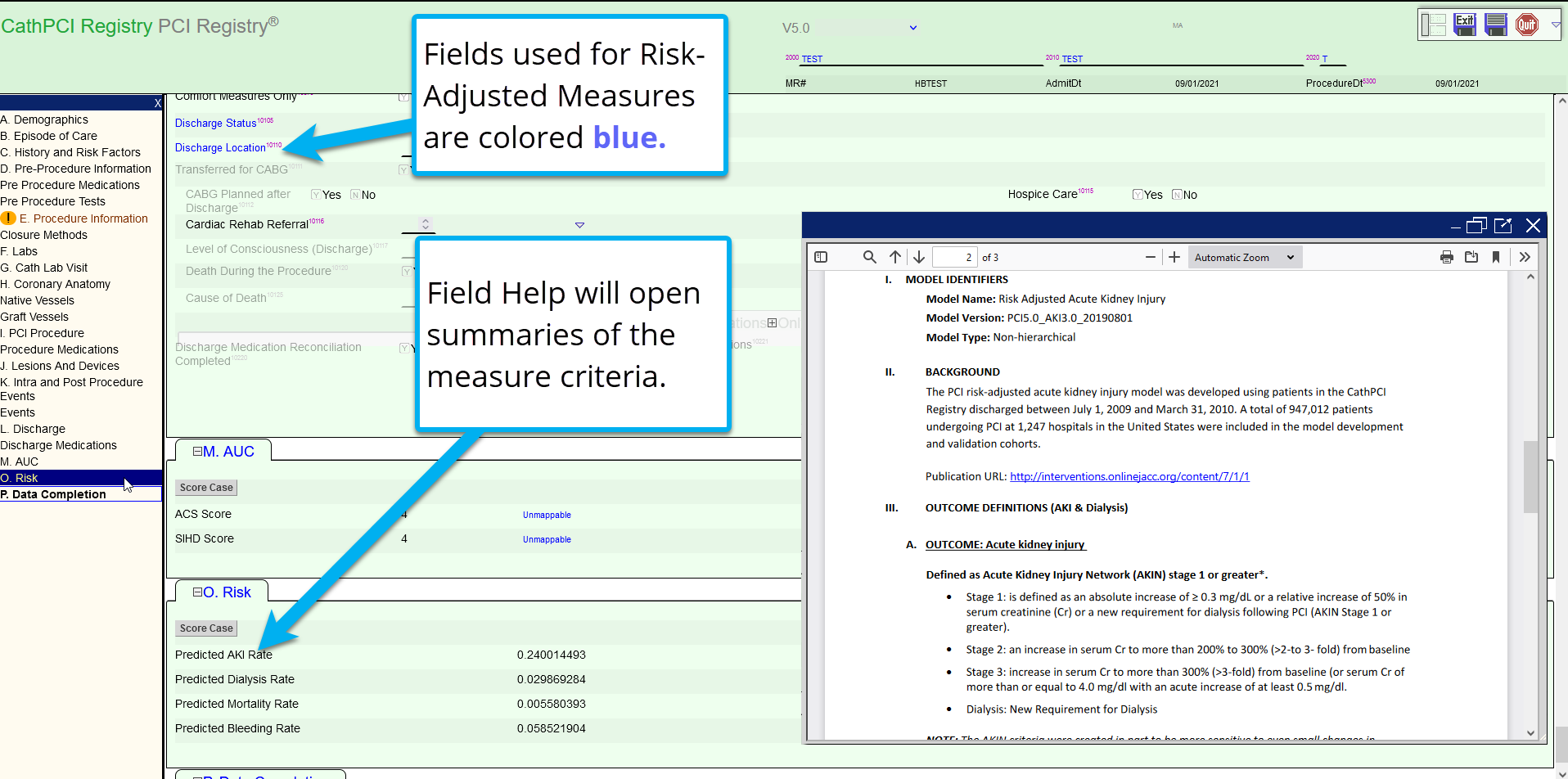 The heartbase platform offers an extensive library of hundreds of clinically meaningful reports, designed to be run by clinical users without the need for special programming knowledge or table joining.
The heartbase platform offers an extensive library of hundreds of clinically meaningful reports, designed to be run by clinical users without the need for special programming knowledge or table joining.
Reports include Officially Licensed Risk Measures, AUC, Executive Measures & NQF Measure Reporting, MD Report Cards, Medication and Equipment Analysis, Complications, and more! Run reports by Network, Region, Hospital, Practice, & Physician, with full patient-level drill-down.
All hbCOR reports are developed through direct collaboration between heartbase and our users. When a user has an idea for a new report, heartbase will work with their facility to build that report free of charge and distribute it to our entire user community during the next report update.
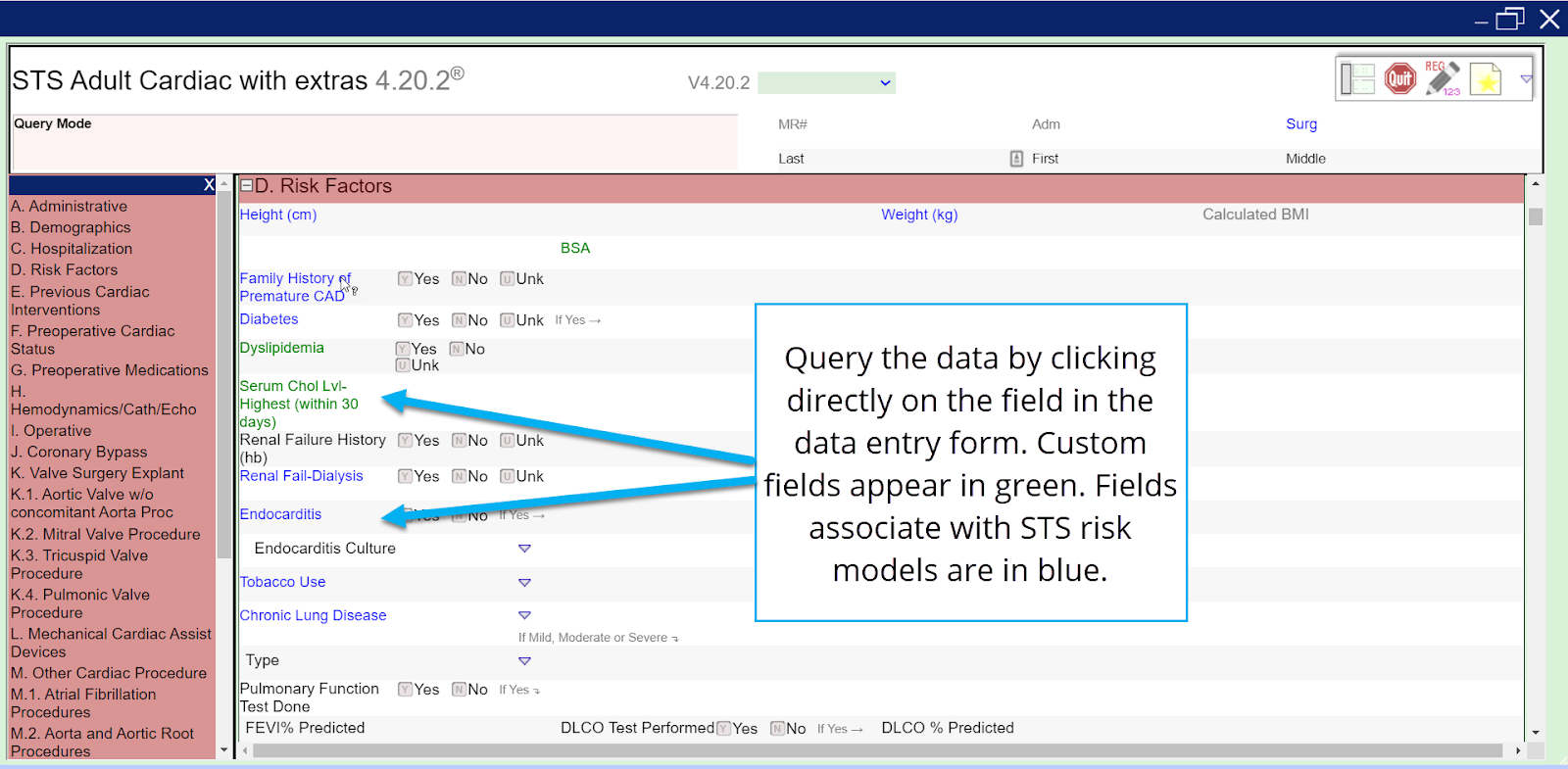 The hbQuery Tool is designed to be easily used by clinical staff, giving them immediate access to all clinical data points in a patient population over any given specified period of time. Heartbase users can select their desired query variables directly from the registry form. The heartbase custom conditional logic tool allows users to filter the values in the hbCOR user interface, rather than manipulating the dataset in a spreadsheet program. Users can easily filter by any field within the registry, including calculated fields such as ProcID (Surgical Operative Category). All custom fields are innately queryable, regardless of what other outputs they are associated with.
The hbQuery Tool is designed to be easily used by clinical staff, giving them immediate access to all clinical data points in a patient population over any given specified period of time. Heartbase users can select their desired query variables directly from the registry form. The heartbase custom conditional logic tool allows users to filter the values in the hbCOR user interface, rather than manipulating the dataset in a spreadsheet program. Users can easily filter by any field within the registry, including calculated fields such as ProcID (Surgical Operative Category). All custom fields are innately queryable, regardless of what other outputs they are associated with.
Query outputs include options for the numeric values as well as the value labels, creating meaningful reports for clinical or statistical users.
The query program can be saved for future use. Saved queries are accessible directly from the heartbase tool and can be run anytime based on a new date range.
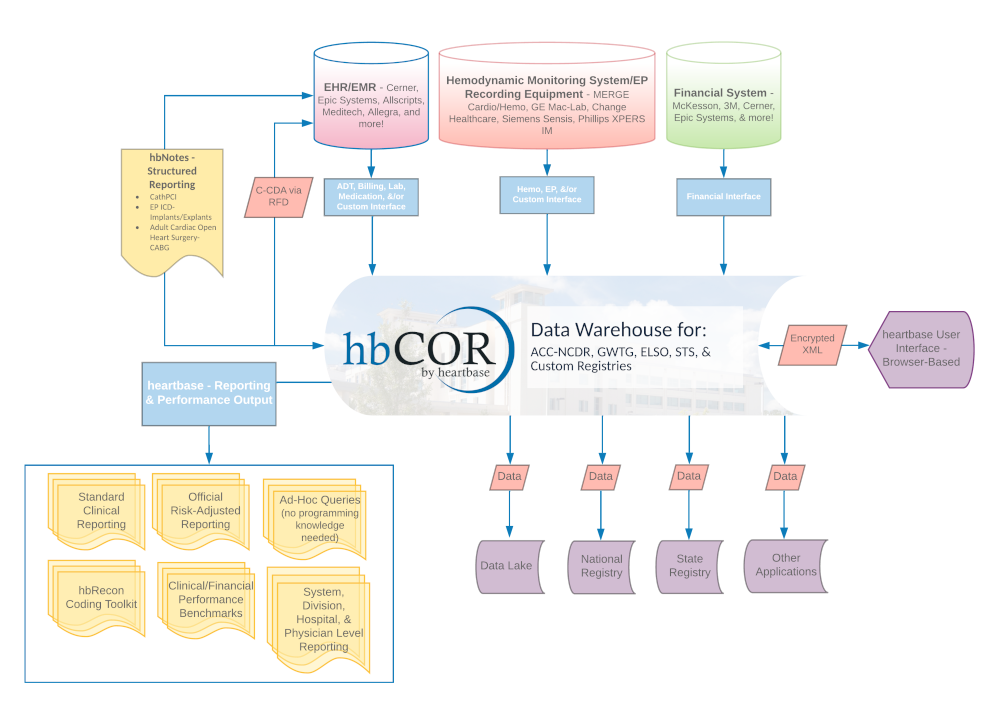
Clinical datasets have become increasingly complex, making it essential for your facility to streamline capture through data sharing and improved system interoperability. Heartbase is uniquely poised to take on the growing challenges of integration due to the distinctive nature of our data model. The heartbase data repository shares all fields with matching data definitions, across all applicable registries and historic versions. With interfaces available from EHRs to hemodynamic monitoring equipment, reducing the burden of manual data collection is available at your fingertips.
As the co-chair of the IHE Cardiology Domain’s Technical Committee, heartbase President Nicholas Gawrit has co-authored several profiles to set standards for interoperability between cardiovascular service lines to streamline data collection,help hospitals meet registry goals, and maximize regulatory compliance.
Beyond our technological solutions, heartbase understands that successful interoperability relies on the human element. We provide the expertise and system flexibility to help your users develop a custom workflow that will ease the burden of data collection and allow them to spend more time analyzing data than entering it.
Registries
-
STS
Adult Cardiac, Congenital, & General Thoracic
-
ACC-NCDR
CathPCI, Chest Pain - MI, EP (ICD & Afib), IMPACT, LAAO, & TVT
-
GWTG, CMS, TJC
GWTG-CAD, HF, Stroke, IQR, OQR, Advanced HF & Stroke Measures
-
State & Custom
CCORP, COAP, PHC4, NYS, NJ, IHA, ELSO ECMO, & Custom Registry Modules
-
hbCOR
Integrated Data Across All Registries & Revisions
- Afib Ablation Versions 1.08 – present
- CathPCI Versions 2.0b – present – Officially Licensed Risk Metrics & AUC
- CP-MI (formerly ACTION) Versions 2.1 – present
- EP Device Implant (Formerly ICD) Versions 1.08 – present
- IMPACT Versions 2.0 – present
- LAAO Version 1.4 (first open to vendors) – present
- STS/ACC TVT Registry Version 3.0 (first open to vendors) – present
Retired Registries
- CARE (Retired) Version 1.09
- PVI (Retired) Version 1.0 – Jan. 2021
- Adult Cardiac Versions 2.35 – present
- Thoracic Versions 2.07 – present
- Congenital Versions 2.3 – present
CMS IP
- Sepsis
CMS OP
- Outpatient ED
- Outpatient STK
- Outpatient MI
The Joint Commission
- VTE
- STK (Not CSTK, but Regular STK)
- Global (ED, IMM, TOB, SUB)
- HBIPS
- PC
- ACHF IP
- ACHF OP
- GWTG CAD Versions Nov. 2017 – present
- GWTG Heart Failure Versions Jan. 2013 – present
- GWTG Stroke Versions April. 2011 – present
State Registries
- California State
- New Jersey State
- New York State
- Washington State
- Pennsylvania State
- Michigan State
- Indiana State
Additional Registries
- ELSO ECMO – First Vendor Certified for Submission
- Custom Registry Development
Interoperability
Interface Functionality: heartbase differs from competitors in the following ways: the heartbase ADT captures all transactions/changes from the admitting system (regardless of registry), rather than having to request the patient from the CVIS. So, as the patient is changed on the Admitting side, that change is also reflected on the heartbase side. This includes Demographics, Admitting, and Discharge information.
Hospital System(s): All EHR vendors.
Registries Affected: All in-scope registries, from 15-36 elements per encounter.
Does this interface create events?: No, this interface only creates up to the encounter level.
Real-time: Yes. As changes are made in the patient record, an ADT message is transmitted to heartbase and immediately consumed.
Interface Functionality: EHRs have the ability to send Abstract Segment (ABS) in parallel with the ADT messages. This allows for real-time coding data to populate the heartbase encounter record.
Hospital System(s):
Registries Affected: Varies site-to-site.
Does this interface create events?: TBD, this interface could be leveraged to create CMS, GTSD, and CP-MI events.
Real-time: Yes. As changes are made in the patient record, an ABS message is transmitted to heartbase and immediately consumed.
Interface Functionality: heartbase requires a batch coding extract for the hbRecon Toolkit & CMS modules.
Hospital System(s): All EHR vendors or coding/quality systems.
Registries Affected: Varies site-to-site.
Does this interface create events?: TBD, this interface could be leveraged to create CMS, GTSD, and CP-MI events.
Real-time: No, typically, a patient is final coded 1-2 weeks post-discharge. These files are typically generated on either a weekly or monthly basis.
Interface Functionality: For the usage of the hbAnalytics Financial Module, including push-button financial reports on associated heartbase data entry screens, the hospital must provide an extract of the required financial information. Heartbase has financial buckets available for the encounter, event, and equipment levels.
Hospital System(s): All EHR vendors or coding/quality systems.
Registries Affected: Varies site-to-site.
Does this interface create events?: No.
Real-time: No, these files are typically generated on either a monthly or quarterly basis.
Interface Functionality: Once a case is closed in the clinical system, the data is automatically routed to a service, which in turn updates the heartbase repository with corresponding discrete data elements.
Hospital System(s): GE Mac-Lab/Cardiolab, MERGE Hemo/Cardio, Philips WITT/XPERS-IM, Change Healthcare, Siemens Sensis, St. Jude, Biotronik, Medtronic, and more.
Registries Affected: ACC-NCDR CathPCI & EP Device Implant. In some cases, these interfaces can be leveraged for other clinical registries.
Does this interface create events?: Yes.
Real-time: No, once a case is closed, the data is automatically routed to a service, which in turn updates the heartbase repository with corresponding discrete data elements.
Interface Functionality: Data from the EHR database, such as Epic Clarity/Caboodle or Cerner Millennium, will be automated via an MFT process to prepopulate registry data within the heartbase application. Using a specification provided by the heartbase team, this interface can be tailored to certain sections of the registry form, such as History & Risk Factors, Medications, and Lab Results. Using an extract versus a standardized interface makes the data selection and validation far more granular and can greatly reduce the data abstraction burden.
Hospital System(s): All EHR vendors.
Registries Affected: Varies site-to-site.
Does this interface create events?: Yes.
Real-time: Varies.
Interface Functionality: heartbase provides custom data lake and third-party extracts based on the needs of the site.
Hospital System(s): Data Lakes and Other Third-Party Systems
Registries Affected: Varies site-to-site.
Does this interface create events?: No, this is an outbound interface.
Real-time: Varies.
Integrating the Healthcare Enterprise (IHE) is an initiative by healthcare professionals to improve hospital system interoperability by engaging clinicians, health authorities, industry, and users to develop, test, and implement standards-based solutions to vital health information needs.
Heartbase President Nicholas Gawrit has served as co-chair of the Cardiology Domain of the IHE Technical Committee since 2014. During his tenure as co-chair he has overseen numerous new standards profiles, including co-authoring the Cardiac Procedure Note (CPN), which consolidated work in the Cath Report Content (CRC) Profile, including Structural Heart Procedures, and the Electrophysiology Report Content Implant/Explant (EPRC-IE) supplement to set standards for interoperability between cardiovascular service lines, streamline data collection to help hospitals meet registry goals, and maximize compliance to MACRA and MIPS. The CPN was developed with a focus on Cath Lab Reports & Electrophysiology Implant and Explant procedures, but aims to provide an extensive framework to allow for the addition of further report templates in the future (e.g., general cardiac imaging procedures like Echocardiography, cardiac CT, MR, or Nuclear Medicine Imaging).